Category Archives: School
A review series on various subjects/topics/lectures we’ve gone over in med school.
OMT: pelvis
This is one of the regions I was assigned to assess for my midterm practical last year. I got off to a wonderful start by handing my grading sheet to my preceptor and smashing my elbow into the corner of the table as I turned to face my patient. We had a good laugh over my misery. :O
Diagnosis:
- Standing flexion test
- SEAT THE PELVIS
- ASIS
- Pubic symphysis
- Inflare/outflare
- SEAT THE PELVIS
- PSIS

Image from “The Pocket Manual of OMT” (2nd ed.).
As usual, ask for contraindications!
- Any recent injuries? Sprains? Fractures?
- Cancer? Infection?
- Arthritis? Joint instability? Hypermobility?
Anterior (aka inferior) innominate ME
- (Supine) Stand on involved side + flex/adduct the hip to its restrictive barrier.
- Pull the buttbone (ischial tuberosity) up.
- Ask pt to push knee into your shoulder for 3-5 seconds against your equal resistance.
- Allow relaxation + move hip to new barrier.
- Repeat 3-5x. Retest.
Posterior innominate ME
- (Supine) Stand on involved side + hold opposite ASIS.
- Move involved leg off the table + let it drop to its extension barrier. (Since it’s posterior, you want your leg to be more posterior, hence why you drop it off the table.)
- Ask pt to push thigh upward for 3-5 seconds.
- Allow relaxation + move hip to new barrier.
- Repeat 3-5x. Retest.
Anterior innominate thrust, supine
- Stand at foot of table and grasp leg above malleoli (use both hands).
- Lift leg to ~30 degrees hip flexion + slightly abduct + internally rotate leg. (Since it’s anterior, you want your leg to be more anterior, hence the flexion.)
- Ask pt to take deep breath. During exhalation, apply a caudad (towards the feet) tug.
- Retest.
Posterior (aka superior) innominate thrust, supine
- (SAME AS ANTERIOR but you don’t flex to 30 degrees.)
Pubic ME, thrust
- Grasp outside of both (flexed) knees. Ask pt to push knees apart for 3-5 seconds. Relax. Repeat 3-5x.
- Separate knees but holding inside of knees with hand/elbow of one arm. Ask pt to push knees together for 3-5 seconds. Relax. Repeat 3-5x.
- Add thrust by applying a short, quick + lateral push at the end.
- Retest.
Ilium inflare ME
- (Supine) Stand on opposite side of inflare + flex knee + hip, putting the foot on the table close to the butt.
- Hold opposite ASIS (the one closest to you) + laterally abduct hip to restrictive barrier.
- Ask pt to push knee medially for 3-5 seconds. Allow for relaxation.
- Repeat 3-5x. Retest.
Ilium outflare ME
- (Supine) Stand on side of outflare + flex knee + hip, putting the foot on the table close to the butt.
- Pull PSIS laterally while medially adducting the hip.
- Ask pt to push knee into external rotation for 3-5 seconds. Allow for relaxation.
- Repeat 3-5x. Retest.
Dracunculus medinensis
- Limited to sub-Saharan Africa
- Ingestion of water w/ larvae
- Matures in abd/retroperitoneal space (1 year later, worm [up to 1 m long] exits body in lower extremity)
- Causes ulceration/erythema at exit site
- Treatment: remove worm by wrapping it around a stick + extracting a few cm per day (speed extraction w/ metronidazole/thiabendazole)
- Classic symbol of medicine (Rod of Asclepius) is said to have come from this treatment
 Interesting. D:
Interesting. D:
OMT: sacrum
I’m pretty sure I’m not the only one, but the day(s) that I know OPP/OMT best tend to be the night before/morning of my practical. We had our midterm practical yesterday, so I figured…what better time to write up my notes on it (while it’s still fresh in my mind and I still remember it!!!) than now?
The sacrum is probably one of my worst sections, so I actually drew something out for it. (What is this sudden dedication!?)
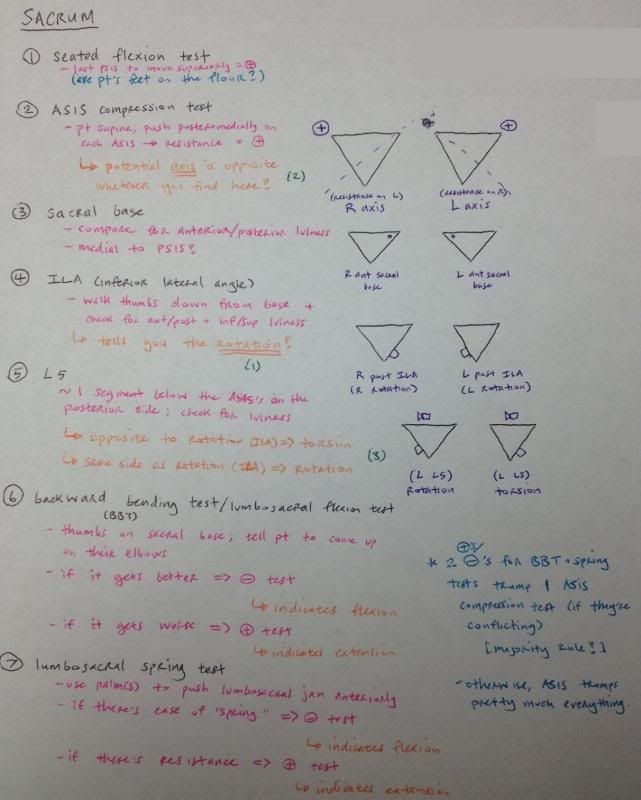
If the answer to the light blue question in #1 is “no,” then you’d best be sure to lower the table until they are. :O

Images from “The Pocket Manual of OMT” (2nd edition).

(The actual diagnostic terminology.)
Sweet! Now that we’ve gotten those out of the way and we have a diagnosis, what next?
Ask about contraindications!
- Have they had any recent injuries to the area?
- Broken bones, fractures, sprains, cancer, infection?
- Arthritis? Blood clots? Possibility of going into premature labor!?
No? Alright, proceed!
But what are you gonna do to make it better? Give me a treatment!
For our midterm, we were responsible for 5 treatments in this section. (I have 5 more sections to write about. It’s gonna be fun.)
Forward sacral torsion ME
- (Lateral Sims) Have pt lie with their problem side (“axis side”) down.
- Since it’s forward, have the pt’s front (their chest) on the table.
- Put one hand on their lumbosacral jxn and flex their hips until you feel motion at the jxn.
- Ask pt to push their feet toward the ceiling for 3-5 seconds against your equal resistance.
- Tell them to relax, then move their legs to the new restrictive barrier.
- Repeat 3-5x. Retest motion/symmetry!
Backward sacral torsion ME
- (Lateral recumbent) Have pt lie with their problem side down.
- Since it’s backward, have the pt’s back on the table.
- Put on hand on their lumbosacral jxn + extend the bottom leg until motion is felt. Bend the top leg + place it behind the other knee.
- Hold shoulder w/ other hand to prevent pt from falling off the table.
- Ask pt to push their flexed knee toward the ceiling for 3-5 seconds against your equal resistance.
- Tell them to relax, then move their legs to the new restrictive barrier.
- Repeat 3-5x. Retest motion/symmetry!
Unilateral sacral flexion ME
- (Prone) Stand facing the pt’s head on side of flexion.
- Place thenar or hypothenar eminence on ILA + push anteriorly/superiorly.
- Use other hand to slightly abduct + internally rotate the leg.
- Ask pt to take a deep breath. Push ILA during inhalation + resist sacral flexion during exhalation.
- Repeat 3-5x. Retest!
Unilateral sacral extension ME
- (Prone) Stand facing pt’s feet on side of extension.
- Place thenar or hypothenar eminence on sacral base + push anteriorly/superiorly.
- Use other hand to slightly abduct + internally rotate the leg.
- Ask pt to take a deep breath. Resist during inhalation + push sacrum into flexion during exhalation.
- Repeat 3-5x. Retest!
Sacroiliac articulatory
- (Lateral Sims) Have pt lie on uninvolved side w/ chest down.
- Stand behind pt + put thenar eminence on sacral base of restricted SI joint + grasp knee w/ other hand.
- Lean in to stabilize, then ask pt to take deep breath + hold it as you flex it to its barrier.
- Slowly abduct + externally rotate hip to barrier + maintain abduction barrier as you extend hip (tell pt to exhale here!).
- Repeat 3-5x. Retest!
test days
We took a really horrible neuro exam the other day that left most of us in depression.
I had dinner with Monika at When Pigs Fly (probably one of my favorite restaurants here :D ). We quizzed each other in neuro and managed to learn everything we needed to about the basal ganglia, dyskinesias and ataxias.
Here are a couple notes, in case you ever want to know a tiny bit more about any of that goodness:
Deep Cerebellar Nuclei (“Don’t Eat Greasy Food”)
- Dentate
- Largest + receives projections from lateral cerebellar hemispheres
- Emboliform + Globose
- Receive input from intermediate part of cerebellar hemispheres
- Collectively known as the interposed nuclei; they’re the inner part of the “sandwich,” so they’re associated with the intermediate hemispheres!
- Fastigial*
- Receives input from vermis + small input from flocculonodular lobe
*Reminds me of the vermiform appendix, which is a vestigial organ, which sounds kinda like fastigial?
Ataxias
- Truncal
- Lesions confined to cerebellar varmis + affect mainly medial motor systems
- Pts w/ lesions of vermis have a wide-based, unsteady drunk-like gait
- Appendicular
- Lesions in intermediate + lateral cerebellar hemispheres + affect lateral motor systems
- Ataxia on movement of extremities (e.g. finger-nose-finger test)
- Sensory
- Occurs when dorsal column/medial lemniscal pathway disrupted
- Loss of joint position sense
- Overshooting limb movements, wide-based unsteady gait (~cerebellar lesion)
- Impaired joint position sense
- Ataxia worse when eyes are closed or in the dark
- Occurs when dorsal column/medial lemniscal pathway disrupted

Beef brisket special w/ steamed kale, a baked sweet potato with cinnamon, horseradish sauce, and a roll.
I got to school super-early the next morning to stake out our usual room so Mike and I could have a mass study-quizzing session. Other than when we had to go into lab, we stayed there for pretty much the entire day. Our lives are really exciting as med students. Sean kidnapped me afterward to make us protein smoothies and deposited us back into our study-home (the catacombs). I came back to find that Mike had come back and left me a message.

He tried to be all sneaky/call my phone so he could get onto it and change my background into a picture of himself, but failed miserably because he didn’t know my passcode. He was a little upset.
We got free breakfast before our exam the next morning, so that was a ray of sunshine in an otherwise dreary morning…

I love the spouse/significant other club. They make/feed us breakfast on exam days. <3
…because despite all the above awesomeness, the exam was horribly demoralizing and I spiraled into a mild depression, so I went to the dog shelter and took several of them on walks to cheer myself up and give em’ some exercise. I had dinner with my study buddies, hung out at their place for a while and ran off to the bike shop to hand out bags to the pre-registered runners for the Zombie Run. Another girl in my class was helping out and we talked whenever there was a lull; I’ve never really interacted with her much, but she’s super nice, so it was cool that I got to know her. She said she thought she might have synesthesia in the sense that she associates different people with animals. To her, I’m apparently a cat!
Tis only fitting, because look at this:

It was impossible to be depressed after this. <3

She looks so content. :]
She brought that up only because a long time ago (she has really good memory o_o), she overheard me saying that someone told me I had a “pouty face” (or that my concentration looked really unhappy) and I responded with, “I can’t help the way my face looks! That’s the way I was born! D:” just to be snarky.






